
Is Your Premature Baby Actually Behind, Or Just Early?
What Actually Happens in Premature Baby Development, Week by Week

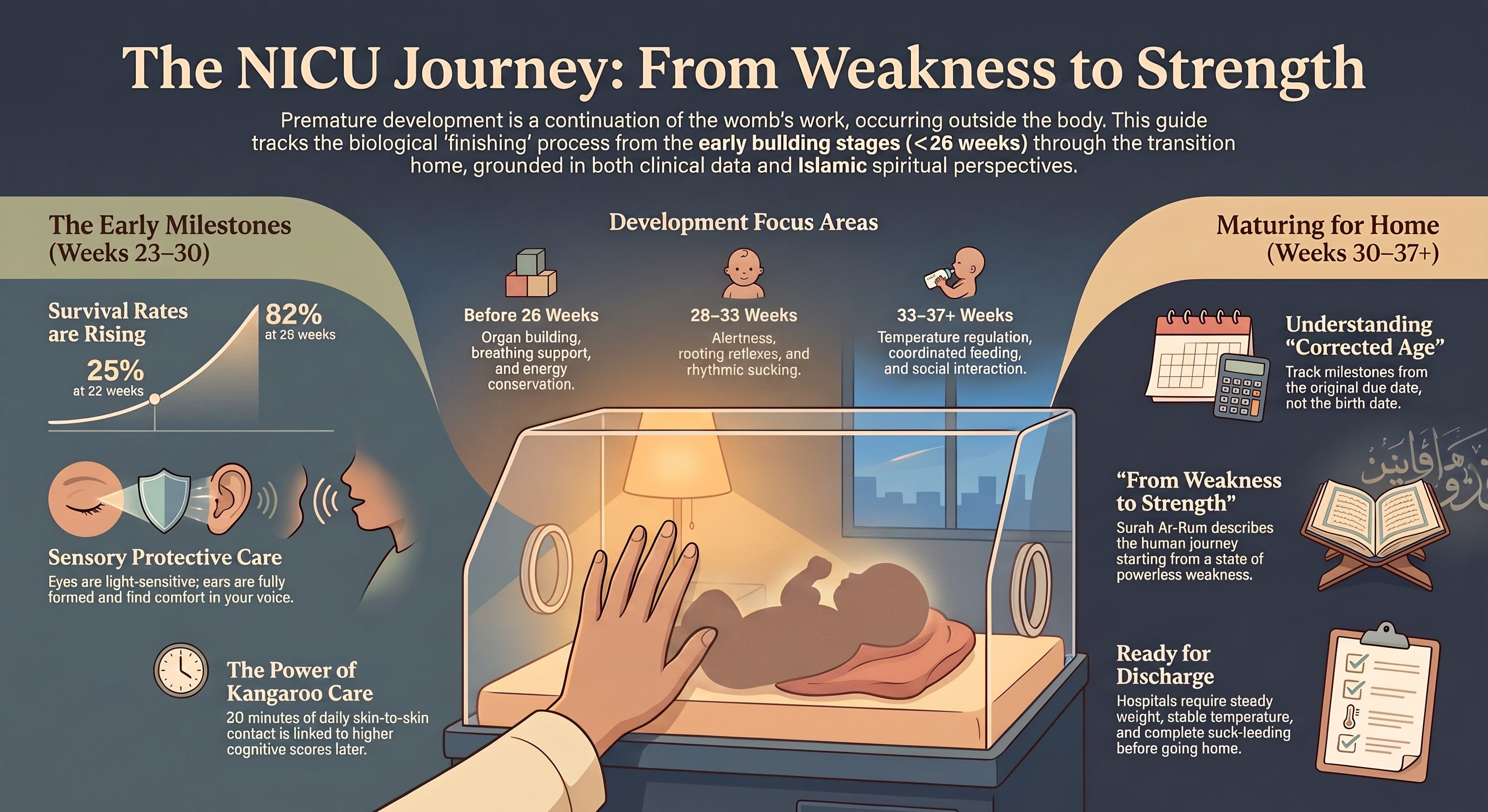
Vermont Oxford Network’s 2024 study tracked over 22,000 NICU infants and found survival climbing from 25% at 22 weeks to 82% at 25 weeks [2] — this guide walks you through exactly what your baby’s body is doing at every stage in between.
Your baby wasn’t supposed to be here yet. Not like this — not wired to monitors, not measured in grams instead of pounds.
Somewhere between one in ten and one in eight babies worldwide arrives before 37 weeks. That’s roughly 13.4 million babies a year [1]. If yours is one of them, you’re not standing outside the normal course of things. You’re standing inside a story shared by millions of parents, in a room that smells like hand sanitizer, waiting for a body that is still, quite literally, being finished.
I’m not going to tell you not to worry. You will worry. But here’s something worth holding onto: your baby’s development hasn’t gone off course. It’s continuing, in the same order it would have followed in the womb, outside the room it was supposed to finish growing in [4].
Why Timing Changes Everything
A baby born at 32 weeks and a baby born at 26 weeks are not on the same road, even though both get called “premature.” The 26-weeker has more ground to cover and, often, more complications along the way by the time they reach 32 weeks — which usually means slower weight gain, a longer road to feeding, and more time before discharge [4].
But medicine keeps closing that gap. Fast.
Why This Guide Is Different From Generic NICU Timelines
Backed by current clinical data. Every developmental stage below reflects 2020–2024 research — including the trial that changed how apnoea of prematurity is treated [9].
Islamic framework woven throughout. This isn’t safety-tips-plus-a-verse-at-the-end — it’s the recognition that Allah’s own words describe exactly what your baby’s body is doing right now.
A tool you’ll actually use. You’ll get a free NICU Journey Companion Pack to keep in your hospital bag — not just information, but something to hold onto at 3am.
Before 26 Weeks: When Everything Is Still Being Built
At 23 weeks, your baby might weigh around 500g and measure about 30cm. By 26 weeks, closer to 750g and 35cm [4].
Their eyelids may still be fused, opening naturally within the first week or so. Once open, they can’t focus, and light itself is genuinely stressful — the NICU environment routinely exceeds the American Academy of Pediatrics’ recommended noise and light thresholds, which is exactly why incubators get covered and lights get dimmed at set times [10]. The ears, though, are fully formed. Your baby can hear you, and may already be sensitive to noise while finding something steadying in your voice — even without any way to respond yet [4].
Touch has to be careful here. Skin marks and bruises easily, and too much handling causes real stress. The care team will tell you when touch becomes appropriate — often within a day or two of birth [4].
Here’s what surprised me researching this: your baby might startle a lot, with jerky, twitchy movements, because their muscles simply aren’t strong enough yet to hold a curled position on their own. Nurses use bedding to support that curled, womb-like posture — not for comfort alone, but because it conserves energy your baby needs for growth [4,6].
Breathing is often the biggest hurdle. The brain’s breathing-control centre isn’t mature, so pauses — apnoea — are common, sometimes needing support for several weeks and occasionally months [4]. Feeding starts through the bloodstream via specially formulated fluid, moving gradually to small amounts of milk delivered through a tube placed in the mouth or nose [4]. Sleep takes up nearly the entire day.
A small practice for this stage: saying Bismillah quietly before any touch — a nappy change, a hand slipped through the incubator porthole — costs nothing and starts a habit that outlasts the NICU by years.
26–28 Weeks: Slow, Steady, Uneven
Weight gain continues, though it may be slow — sometimes from illness, sometimes because feeding has to be introduced in careful, staged amounts to protect a digestive system that isn’t ready for more [4]. Eyes may open now, though coordinated focus is still out of reach; eyelashes and eyebrows begin growing in, and blinking starts. Reactions to sound can shift hour to hour, which is actually useful — it’s your baby beginning to show you what soothes and what overwhelms [4].
Muscles are still developing, so twitches and tremors are entirely normal here. If your baby is medically stable, skin-to-skin (kangaroo) care can often begin — prioritise it. A 2024 Stanford Medicine study found each additional 20 minutes of daily skin-to-skin contact was linked to a 10-point rise on a standardised cognitive scale at 12 months, independent of gestational age [3]. Breathing support is usually still needed. Sucking movements may appear, but true suck-feeding stays out of reach — it requires breathing, sucking, and swallowing to work in coordinated sequence, and that sequence isn’t ready [4].
28–30 Weeks: The First Real Alertness
Bright light now makes your baby squeeze their eyelids shut, though moving both eyes together is still limited — worth remembering when thinking about the light around the incubator. Pleasant sounds get a response, and your baby may seem to “wake up” specifically for your voice during their brief alert windows. Offering one form of stimulation at a time — quiet Qur’an recitation or eye contact, not both together — tends to work better than combining them [4].
Movement becomes more active as muscles strengthen, though good positioning support still matters [4,6]. Around now, the rooting reflex — turning toward a touch on the cheek — often emerges, an early building block toward feeding; some babies at this stage can manage sucking on a cotton bud dipped in milk, even though a real feed is still out of reach [4]. Sleep starts organising into recognisable deep and light phases, with the first genuine short alert periods appearing, their length shaped by your baby’s health, the environment, and even the time of day [4].
30–33 Weeks: Finding a Rhythm
Babies born at this point may need relatively little medical intervention, though they still need time in hospital to mature [4]. Movements smooth out and become more controlled; limbs settle into a more bent, natural position. Because touch sensitivity is often still high, narrating what’s about to happen — “I’m changing your nappy now” — helps your baby start linking your voice to safety [4,7].
Rhythmic sucking frequently begins here, and letting your baby smell and taste breastmilk, or gently touching their lips and the inside of their mouth before feeds, can help prepare their senses for what’s coming [4]. Deep sleep increases, and alert periods lengthen — especially in a dim room — often centred on your face or another interesting object, with your baby possibly responding to your voice. You may start noticing your baby’s first attempts at self-soothing, like bringing a hand to their mouth — one of the clearest signs of comfort at this stage [4].
33–36 Weeks: Almost There
Close to term now, though still not quite behaving like a full-term newborn. Responses to sound become consistent enough that you’ll start predicting them day to day. Movement is smoother and more deliberate; your baby can hold their limbs where they choose and turn their head from side to side as their muscles strengthen [4]. Touch sensitivity often lingers, so continuing to narrate care still helps.
Apnoea has usually resolved by now, sometimes with the help of caffeine therapy — a treatment shown in a landmark international trial to meaningfully reduce apnoea episodes and the need for mechanical ventilation in very low birthweight infants [9]. Suck-feeding — breastfeeding, where possible, considered ideal for premature babies — typically becomes achievable [4]. Sleep and wake states sharpen into distinct categories: quiet sleep, active sleep, drowsy, alert, fussy, crying. Social alert periods lengthen, and your baby gains the ability to turn away or close their eyes when they’ve had enough — that’s communication, not withdrawal [4]. Crying stays infrequent here but increases the closer your baby gets to term.
37 Weeks and Beyond: Getting Ready to Go Home
Some babies go home before their original due date. Others — especially those born very early or with medical complications — need longer. Hospitals typically look for steady weight gain, a stable body temperature outside the incubator, complete suck-feeding, and the absence of apnoea before clearing a baby for discharge [4].
One thing worth knowing now: your baby’s corrected age — counted from their original due date, not their birth date — matters more than the calendar for the first two to three years. A baby born eight weeks early isn’t behind a full-term baby at three months. They’re a newborn who happens to be three months old on paper. I know it’s tempting to compare your baby’s NICU chart to a friend’s full-term baby book anyway. Try not to. It’s not the same book.
I know this is a lot to hold, especially when you’re running on hospital coffee and hourly updates. That’s why I’ve created a free NICU Journey Companion Pack — a printable guide with a stage-by-stage milestone card, a corrected-age tracker, and something to carry you through the waiting. Keep reading to download it at the end — it’s designed to stay in your hospital bag, where this actually happens.
The Islamic Framework For Premature Baby Development: Born Weak, Growing Strong
As Muslim parents, it can help to remember our children’s bodies were never entirely in our hands — not even in the womb. When I sit with the verse where Allah says, “Allah is the one who created you from weakness, then made after weakness strength, then made after strength weakness and white hair” [12], I think about how directly it describes what’s happening in that incubator. According to Tafsir Ibn Kathir, this verse traces the entire arc of a human life, beginning with the moment a person “emerges from his mother’s womb, weak and thin and powerless,” before growing “little by little” into strength. Your baby isn’t deviating from that design. They’re living it, more visibly than most of us ever see up close.
There’s a companion comfort in something the Prophet ﷺ said: “There is no disease that Allah has created, except that He also has created its treatment” [13]. Every scan, every specialist, every ventilator adjustment, every dose of caffeine to steady a breathing rhythm — these are means Allah placed in the world for exactly this moment. Using them fully isn’t a lack of tawakkul. It’s tawakkul lived out, through the hands of the people Allah sent to your baby’s bedside.
Weakness was never a flaw in the design. It’s the beginning of it.
If you’ve read this far, you’re the kind of parent who wants to understand what’s happening to your baby, not just survive the waiting. That tells me something beautiful about you.
Inside the NICU Journey Companion Pack (one comprehensive PDF, 3 pages):
Page 1: The Gestational Stage Quick-Reference Card — A visual guide covering every stage from “before 26 weeks” through “37 weeks and beyond,” showing what’s developing and what to expect at each point — designed as a card you can keep in your hospital bag or clipped to the incubator.
Page 2: Corrected Age & Conversation Tracker — A simple tool for calculating your baby’s corrected age at any point in their first two years, plus a running space to jot questions for rounds, so you can walk into every conversation with your baby’s care team prepared, not scrambling.
Page 3: A Reminder for the Waiting — The Prophet ﷺ’s teaching on how “wondrous is the affair of the believer” [14], paired with the weakness-to-strength verse from Surah Ar-Rum, formatted as something you can tape to the wall beside the incubator on the hard days.
This isn’t just a PDF to download and forget. It’s a tool designed to stay in your hospital bag — where you’ll actually reach for it when you need it most.
This companion pack is what every subscriber receives with each article. We cover the full journey of raising Muslim children, all backed by scientific research and rooted in Islamic wisdom.
If you’re a Muslim parent who wants both evidence-based guidance and Islamic perspective, subscribe for free so future resources arrive in your inbox before you need them.
Subscribe free for parenting resources backed by both science and Sunnah — no spam, no clutter, just resources that matter when you need them.
Let’s Start With A Small Action
Before you keep scrolling, do this: save this article, or screenshot the week-by-week sections. The next time a nurse mentions a milestone you don’t recognise, you’ll have language for it already in your pocket.
May Allah place barakah in every gram gained, ease in every long night, and make this waiting shorter than it feels right now, ameen!
Think of Someone Who Needs It
Think of one person right now: the friend whose baby shower got replaced by a NICU visit, the sister-in-law who’s been posting hospital photos without much explanation, the mother at the masjid you haven’t seen in weeks because she hasn’t left the hospital.
This article could be the thing that helps them make sense of what their baby’s body is doing. Share it with them today — not because you’re being preachy, but because you care. Sometimes the most loving thing we can do is pass along understanding at a moment when everything feels unexplainable.
Frequently Asked Questions
Q: What is considered a premature baby?
A: Any baby born before 37 completed weeks of pregnancy [1]. Prematurity is further divided into extremely preterm (before 28 weeks), very preterm (28–32 weeks), and moderate to late preterm (32–37 weeks).
Q: What is corrected age, and how long do I use it?
A: Corrected age is your baby’s age counted from their original due date, not their birth date. Doctors typically use it for the first two to three years, longer for extremely premature babies. See “37 Weeks and Beyond” above for why it matters more than the calendar.
Q: How long does a premature baby usually stay in the NICU?
A: It varies by gestational age and complications, but many babies stay until close to their original due date. Hospitals generally look for steady weight gain, stable temperature, full suck-feeding, and no apnoea before discharge [4].
Q: Is skin-to-skin (kangaroo) care safe for a premature baby on monitors?
A: Yes, when cleared by your baby’s medical team — many babies on monitors and even respiratory support can still do it. It’s one of the most evidence-backed things you can do; each extra 20 minutes daily has been linked to measurably better cognitive outcomes at one year [3].
Q: Why is caffeine given to premature babies?
A: Caffeine citrate stimulates the breathing-control centre in the brain and is a standard, well-studied treatment for apnoea of prematurity — a major international trial found it reduced apnoea episodes and the need for mechanical ventilation in very low birthweight infants [9].
Q: Will my premature baby catch up developmentally to full-term babies?
A: Most do, especially babies born after 28 weeks, though the timeline varies. Using corrected age rather than birth age is the most accurate way to track this, and your baby’s care team can guide you on individual expectations.
References
[1] World Health Organization (WHO). (2023–2024). Preterm birth fact sheet. https://www.who.int/news-room/fact-sheets/detail/preterm-birth
[2] Vermont Oxford Network / American Academy of Pediatrics. (2024). Survival of Infants Born at 22 to 25 Weeks’ Gestation Receiving Care in the NICU: 2020–2022. Pediatrics, 154(4). https://publications.aap.org/pediatrics/article/154/4/e2024065963
[3] Scala, M., et al. (2024). Skin-to-skin care and neurodevelopmental outcomes in preterm infants. Journal of Pediatrics, reported in Stanford Medicine (2024). https://www.sciencedaily.com/releases/2024/08/240807225610.htm
[4] Altit, G., Hamilton, D., & O’Brien, K. (2024). Skin-to-skin care (SSC) for term and preterm infants. Paediatrics & Child Health, 29(4), 238-245. https://doi.org/10.1093/pch/pxae015
[5] World Health Organization (WHO). WHO recommendations for care of the preterm or low-birth-weight infant. https://www.who.int/publications/i/item/9789240058262
[6] Madlinger-Lewis, L., Reynolds, L., Zarem, C., Crapnell, T., Inder, T., & Pineda, R. (2014). The effects of alternative positioning on preterm infants in the neonatal intensive care unit: A randomized clinical trial. Research in Developmental Disabilities, 35(2), 490-497. https://doi.org/10.1016/j.ridd.2013.11.019
[7] Øberg, G.K., Blanchard, Y., & Obstfelder, A. (2014). Therapeutic encounters with preterm infants: Interaction, posture and movement. Physiotherapy Theory and Practice, 30(1), 1-5. https://doi.org/10.3109/09593985.2013.806621
[8] Wechsler Linden, D., Trenti Paroli, E., & Wechsler Doron, M. (2010). Preemies: The essential guide for parents of premature babies (2nd edn). Simon & Schuster.
[9] Schmidt, B., Roberts, R.S., Davis, P., et al. (2006). Caffeine therapy for apnea of prematurity. New England Journal of Medicine, 354(20), 2112-2121. https://doi.org/10.1056/NEJMoa054065
[10] Almadhoob, A., & Ohlsson, A. (2020). Sound reduction management in the neonatal intensive care unit for preterm or very low birth weight infants. Cochrane Database of Systematic Reviews; American Academy of Pediatrics Committee on Environmental Health noise/light thresholds (45 dB / 600 lux). https://pmc.ncbi.nlm.nih.gov/articles/PMC6989790/
[11] Neu, M., Robinson, J., & Schmiege, S.J. (2013). Influence of holding practice on preterm infant development. MCN: The American Journal of Maternal Child Nursing, 38(3), 136-143. https://doi.org/10.1097/NMC.0b013e31827ca68c
[12] Qur’an, Surah Ar-Rum 30:54 — https://quran.com/30/54 — with Tafsir Ibn Kathir: https://quran.com/30/54/tafsirs/en-tafisr-ibn-kathir
[13] Sahih al-Bukhari 5678 — Graded: Sahih — https://sunnah.com/bukhari:5678
[14] Sahih Muslim 2999 — Graded: Sahih — https://sunnah.com/muslim:2999