
Most Parents Don't Know These Speech Warning Signs Until It's Too Late
The "Wait And See" Mistake Parents Make With Speech Disorders

1 in 12 children aged 3–17 has a speech or voice disorder. [1] Most parents are told to wait and see. But research consistently shows that children who receive early speech pathology support do significantly better than those who don’t. [10] Here’s how to tell the difference and what to do either way.
Your child is trying to tell you something. You lean in. You listen hard. And still — you can’t quite catch it. They say it again, a little louder. Their eyes find yours.
That moment — where a child can’t make themselves understood — is one of the quieter hard things in parenting. Not dramatic. Just persistent.
Here’s what I wish more parents knew before they started worrying, or before they stopped: there is a specific line between normal speech development and a speech disorder — and it’s clearer than most people think. Most early errors are not just expected, they’re necessary. They’re how the developing system works. But some patterns genuinely do need attention, and recognising them early makes a real difference.
When I studied the national data on speech and communication disorders, one number stayed with me: approximately 1 in 12 children between ages 3 and 17 has a speech or voice disorder. [1] That’s not unusual. That’s a child in nearly every classroom. And the research from the Cochrane Database is consistent: early speech pathology intervention produces significantly better outcomes than watchful waiting when a genuine disorder is present. [10]
You don’t need to panic. But you do need to know what you’re looking for.
Why This Guide Is Different
Research-backed, not reassurance: Every milestone, benchmark, and sign of concern in this guide comes from peer-reviewed speech science — not generic “they’ll grow out of it” advice.
Islamic wisdom woven throughout: This isn’t just developmental information. It’s grounded in the Sunnah model of clear, deliberate, unhurried speech — and what it means to care for your child’s tongue as an amanah from Allah.
A printable tool to take with you: You’ll receive the When Sounds Take Longer: Speech Development Companion Pack — a free 3-page PDF with a sound-by-age reference card, a home support strategy sheet, and a family tarbiyah practice card built around the Qur’anic concept of tartil.
What Normal Speech Development Actually Looks Like
Children are supposed to make errors. This is worth saying plainly, because so much parenting anxiety around speech comes from treating errors as warning signs when they’re actually milestones.
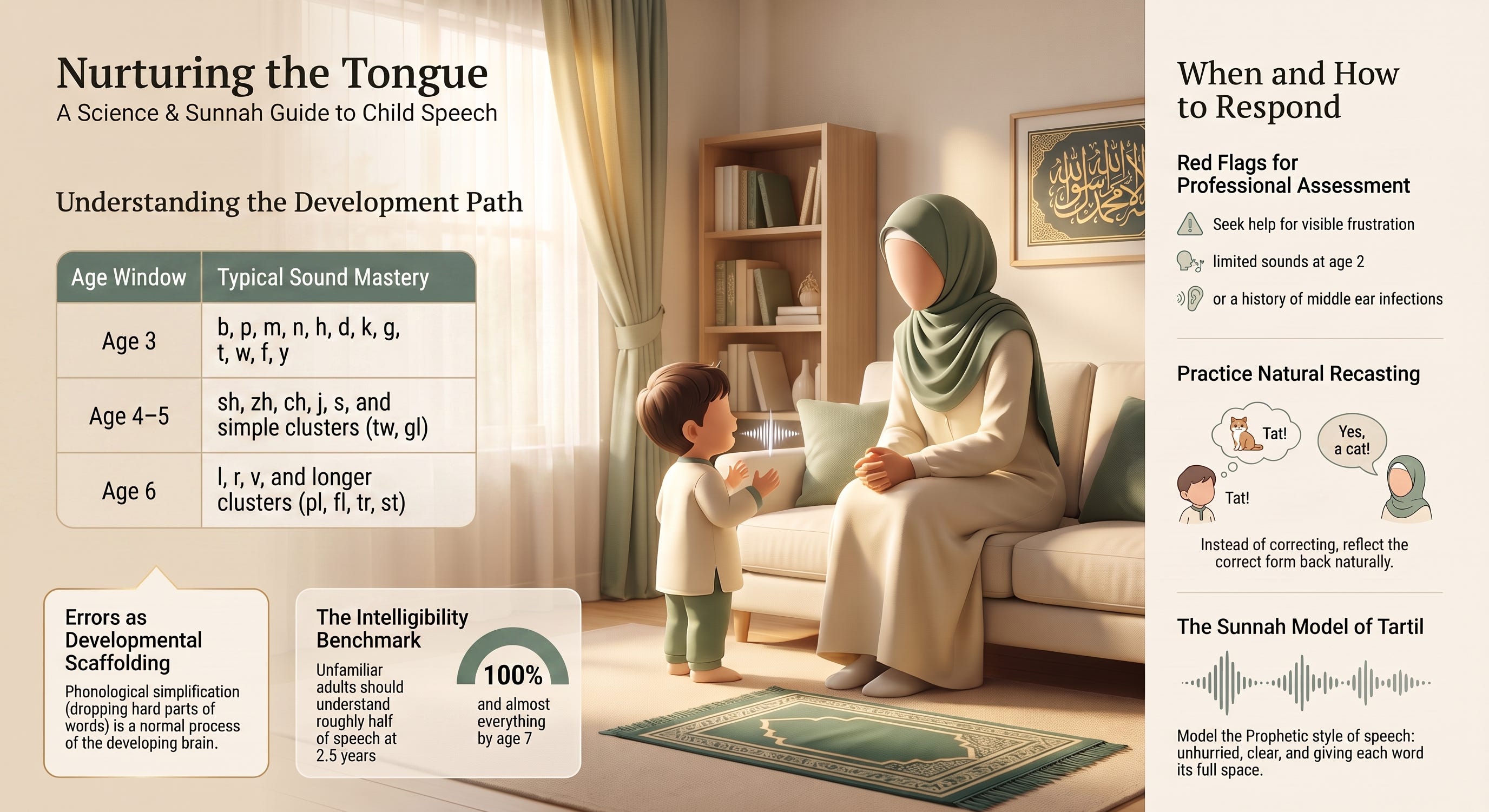
Children simplify. They substitute sounds they can’t yet produce with ones they can. They drop the hard parts and keep the manageable ones. This is called phonological simplification — and it’s not a problem, it’s a process. [2, 3] The developing brain produces speech in stages, and errors are the scaffolding.
What matters is whether the errors match the expected stage.
Here’s when most children master specific sounds [2, 3, 4]:
Around age 3: b, p, m, n, h, d, k, g, t, w, f, y
Ages 4–5: sh, zh, ch, j, s, and simple consonant clusters like tw, kw, gl, bl
Age 6: l, r, v, and longer clusters including pl, kl, kr, fl, tr, st, dr, br, fr, gr, sn, sk, sw, sp, str, spl
Ages 7–8: th, z, and complex clusters like sm, sl, thr, skw, spr, skr
And a guide to how much of a child’s speech an unfamiliar adult should be able to understand [4, 5]:
At 2.5 years: roughly half
At 4–5 years: most of it, with some errors still present
At 6–7 years: almost everything, with possible difficulty only on late-developing sounds like th
If your child is within these windows — even with noticeable errors — you almost certainly don’t need to do anything differently. The errors themselves are information, not failure.
What a Speech Disorder Actually Is — and What It Isn’t
A speech sound disorder is specifically about how sounds are physically produced — not about vocabulary, grammar, or understanding language. That distinction matters.
Language delay is when a child has difficulty understanding or using spoken language itself: their vocabulary, sentence structure, comprehension. A speech disorder is when the physical production of sound — the coordination of lips, tongue, teeth, jaw, soft palate, and breath — is significantly more difficult or inaccurate than expected for the child’s age. A child can have one without the other, and the two require different kinds of support. [6, 9]
Speech sound disorders generally fall into these categories:
Articulation difficulties — consistently producing specific sounds incorrectly, beyond the age when that error should have resolved. The classic example: a six-year-old who always says “wabbit” for “rabbit,” long past the age when that substitution is typical.
Phonological disorders — systematic error patterns affecting whole classes of sounds. A child who consistently drops the final consonant from every word (”ca-” for “cat,” “cu-” for “cup”) isn’t making random errors — they’re following an internal rule that needs to be restructured. Identifying the pattern is key to knowing how to help. [6]
Fluency difficulties — including stuttering: repetitions of sounds or syllables, prolonged sounds, or blocks where speech gets stuck. Dysfluency in children aged 2–5 is very common and often resolves on its own. Persistent, severe, or distressing stuttering warrants a professional assessment. [6, 9]
Signs That Are Worth Acting On
Most speech concerns can be safely monitored. But these signs genuinely warrant reaching out to a paediatrician or speech pathologist sooner rather than later [5, 7]:
Speech that is consistently difficult to understand — even for you — beyond what’s typical for the child’s age
Visible frustration, avoidance of speaking, or distress when not understood
Very limited speech sounds at two years of age
Repetitions, getting stuck, or speech that requires significant effort
Repeated middle ear infections, a history of glue ear, or any concerns about hearing
That frustration piece. Don’t talk yourself out of it. A child who is upset about not being understood is signalling something real — with the very system that’s struggling. That signal deserves a response. Not just reassurance. A response.
And on the question of when: the right time to seek assessment is when you’re concerned. Not when the concern becomes severe. Not when the nursery teacher finally raises it formally. An assessment gives you one of two things — reassurance that development is on track, or early identification that opens a pathway forward. Both are worth having. [7, 9]
I know keeping track of all of this is a lot, especially when you’re trying to stay present rather than constantly evaluating. That’s exactly why I created the When Sounds Take Longer: Speech Development Companion Pack — a free 3-page printable with a sound-by-age reference card, a home support guide, and a tartil family practice card. Keep reading to download it at the end.
What Causes Speech Disorders and What Doesn’t
Here’s something worth saying clearly: most speech disorders have no single identifiable cause. And there is nothing most parents could have done differently to prevent them. [2, 5] Guilt finds parents wherever there’s uncertainty — and it isn’t helpful here.
Known factors that can be associated with speech disorders include:
Structural differences — a cleft palate or other oral differences that directly affect how sounds can be physically formed.
Hearing difficulties — this connection is more significant than many parents realise. What the ear cannot clearly distinguish — the fine differences between p and b, between f and v, between voiced and unvoiced consonants — the mouth cannot reliably learn to produce. Persistent glue ear from repeated middle ear infections is one of the most common and treatable contributors to speech sound difficulties. [7, 9] If hearing is in question alongside speech concerns, both should be assessed together.
Genetic factors — some genetic conditions are associated with a higher prevalence of speech difficulties.
Co-occurring developmental differences — speech disorders occur more frequently alongside autism spectrum conditions and ADHD, though the presence of one does not confirm the other. [5, 9] Assessment should always look at the full picture.
In many cases — probably most — none of these factors will be present and the cause will remain unclear. That doesn’t make the difficulty less real or less treatable.
The Sunnah Model: Clear, Deliberate, Patient Speech
When I think about what the Prophet ﷺ modelled in his own communication, I keep returning to something Aisha (رضي الله عنها) preserved for us in Sahih al-Bukhari: that he spoke so clearly that if someone wanted to count his words, they could. [8]
Unhurried. Each word given its full space. This is not just a description of eloquence — it’s a description of deliberateness. And it is, almost exactly, what the research tells us children’s developing phonological systems most need from the adults around them.
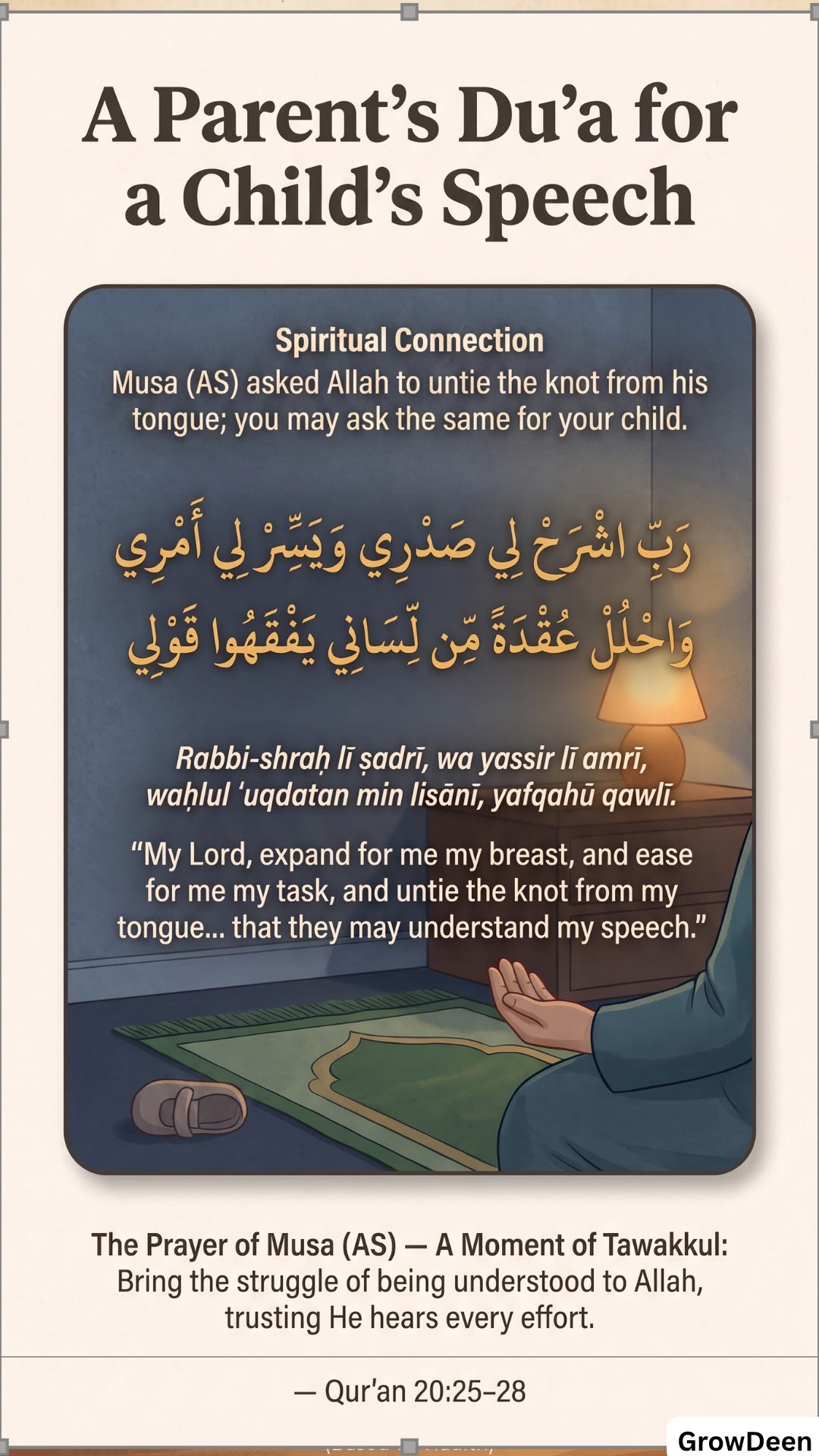
Allah commands in Surah Al-Muzzammil: “...and recite the Qur’an with measured recitation (tartilan).” [1-Q] According to Tafsir Ibn Kathir, tartil means giving each letter its due from its correct articulation point (makhraj) — slowly, clearly, without rushing. Ali ibn Abi Talib (رضي الله عنه) defined it as delivering each word from its proper place of articulation. This is the science of speech, written into our recitation practice centuries before speech pathology existed as a field.
When we model slow, clear, deliberate speech with our children — when we make Qur’an recitation part of the daily sound environment, when we say Bismillah audibly before small acts, when we narrate what we’re doing in clear, unhurried language — we are doing tarbiyah and speech support in the same breath.
And when we notice that support is needed, and we take the step to find it — that too is part of the trust.
May Allah place barakah in every sound your child is still learning to form.
How to Support Your Child’s Speech at Home
The most effective home strategy is not correcting — it is modelling. Here’s why that distinction matters.
Constant correction increases anxiety around speaking, and speaking anxiety typically makes production worse. What the research consistently supports is natural recasting: reflecting back the correct form as a natural part of the continuing conversation. [9]
If your child says, “I saw a tat!” — you say: “A cat! Where was the cat? What was it doing?” The word “cat” is there. Offered clearly, warmly, as part of connection — not as a lesson.
Other strategies that make a genuine difference [9, 10]:
Give them unhurried time. Eye contact, body turned toward them, no finishing their sentence before they’ve reached it. A child who feels rushed produces more errors. A child who feels your full attention takes the risk of trying.
When you can’t understand, open a door rather than ask them to repeat. “Can you show me?” “Is it something from this morning?” “Is it the red one?” This keeps communication moving without asking them to repeat what they’ve already found difficult.
Surround them with clear, deliberate language. Qur’an recitation played at home, du’a made audibly before meals, stories narrated across the dinner table — a home filled with careful, unhurried language is already doing something powerful for a child’s phonological development, whether or not any professional support is ever needed.
Read aloud together. Stories, Islamic books, the names of things you pass during the day. The steady, warm stream of clearly produced adult speech is among the strongest environmental inputs in early speech development. [9, 10]
Your Free Companion Pack
If you’ve read this far, you’re the kind of parent who takes their child’s development seriously — not out of anxiety, but out of love. That says something.
Inside the When Sounds Take Longer: Speech Development Companion Pack (one comprehensive PDF, 3 pages):
Page 1: Speech Sounds by Age — Quick Reference Card — A clean, printable chart showing when each sound is typically mastered from age 3 through 8, what errors are still normal at each stage, a simple “is this typical?” checklist, and the three key signs that warrant a professional assessment — designed as a card you can keep in your child’s folder, on the fridge, or take to paediatrician visits.
Page 2: Supporting Speech at Home — A Parent’s Strategy Sheet — The key do’s and don’ts of home speech support: how to use natural recasting in real conversations, how to respond when you can’t understand, how to build a language-rich environment using your daily Islamic routines, and what to say when booking a first assessment — formatted as a practical, scannable reference you’ll actually return to.
Page 3: Tartil in Our Home — A Family Tarbiyah Practice Card — A beautifully designed card centred on Qur’an 73:4 (wa rattil al-Qur’āna tartīlā) in full Arabic script, with transliteration and translation, plus five Sunnah-rooted daily practices for modelling deliberate, clear speech in your home — from how you recite before sleeping to the care you bring to speaking with your child.
This isn’t a PDF to download once and forget. It’s a tool designed to stay on your fridge or in your child’s folder — where you’ll actually find it when you need it.
Muslim Parenting Lab covers the full journey of raising Muslim children — from how sounds form in the first years of life, through body safety conversations, teenage challenges, and everything in between. All of it backed by research. All of it rooted in Islamic wisdom.
If that’s what you’re looking for, subscribe free so the next resource reaches you before you need it.
Subscribe free for parenting guidance backed by both science and Sunnah — the kind of depth you genuinely can’t find anywhere else. No spam, no clutter, just what matters.
One Thing to Do Right Now
The next time your child says something you can’t quite catch: don’t ask them to repeat it the same way. Instead, try opening a door. “Can you show me?” “Is it the blue one?” Give them a different path to the meaning. That one shift — today, in your next conversation — is already the practice.
Share This with Someone Who Needs It
Think of one person right now: the mother in your WhatsApp group who mentioned her three-year-old isn’t very clear yet and everyone said “give it time.” The sister whose child’s nursery teacher raised something last term and she hasn’t quite known what to do with it. Someone who is quietly worried but hasn’t said so — because they don’t know if the worry is justified.
This article might give them exactly what they’ve been looking for. Share it with them — not as a diagnosis, but as company. Sometimes the most loving thing we can do is pass along knowledge that removes the weight of not knowing.
Frequently Asked Questions
Q: How do I know if my child has a speech disorder or is just a late talker?
A: These are actually two different concerns. Late talking typically refers to limited vocabulary or language use — a child who isn’t saying many words for their age. A speech disorder is specifically about how sounds are produced — a child may talk plenty but be difficult to understand. If your child’s speech is hard to follow consistently, beyond what’s typical for their age, that points toward a speech sound concern worth assessing. For age-by-age benchmarks, see “What Normal Speech Development Actually Looks Like” above.
Q: At what age should I be worried about my child’s speech?
A: The key is always whether errors match what’s expected at that specific age — not age alone. A useful benchmark: an unfamiliar adult should understand roughly half of what a 2.5-year-old says, and most of what a 4–5-year-old says. [4, 5] But visible frustration — your child’s clear distress at not being understood — is a signal I’d always respond to, regardless of age.
Q: Can speech disorders be caused by hearing problems?
A: Yes, and this link is more significant than many parents realise. [7, 9] What the ear can’t clearly distinguish, the mouth can’t reliably learn to produce. Repeated middle ear infections causing temporary hearing loss — glue ear — are one of the most common and treatable contributors to speech sound difficulties. If hearing has been a concern alongside speech, ask for both assessments at the same time.
Q: What does a speech pathology session with a young child actually look like?
A: For young children, sessions are almost always play-based — books, games, and targeted activities that build the specific sounds the child needs. [9, 10] It’s not drills or clinical exercises. Parents are usually coached on what to do between sessions at home, which significantly speeds up progress. The combination of regular sessions and daily home practice is what the research supports.
Q: My child is bilingual. Does that affect speech development?
A: Bilingualism does not cause speech disorders and doesn’t typically delay speech sound acquisition. [9] It can create a slightly wider window of variation for some sounds, since the child’s phonological system is learning two languages simultaneously. A thorough assessment should always account for both languages — a good speech pathologist will ask about home language use before drawing any conclusions.
Q: Is stuttering a speech disorder? Do I need to act on it?
A: Dysfluency — repetitions, prolongations, getting stuck — is extremely common between ages 2–5 and often resolves without any intervention. [6] It spikes when children are excited, tired, or when their ideas outpace their ability to produce them. If it persists past age 5, causes visible distress, or comes with physical struggle like facial tension, an assessment is a sensible step. You don’t need to treat it as a crisis — but you don’t need to dismiss it if it’s persisting and your child is clearly bothered by it.
References
[1] National Institute on Deafness and Other Communication Disorders (NIDCD). (2021). Quick statistics about voice, speech, language. U.S. Department of Health and Human Services. https://www.nidcd.nih.gov/health/statistics/quick-statistics-voice-speech-language
[2] Baker, E., & McLeod, S. (2011). Evidence-based practice for children with speech sound disorders: Part 1 narrative review. Language, Speech, and Hearing Services in Schools, 42(2), 102–139. https://doi.org/10.1044/0161-1461(2010/09-0075)
[3] Dodd, B., Holm, A., Hua, Z., & Crosbie, S. (2003). Phonological development: A normative study of British English-speaking children. Clinical Linguistics & Phonetics, 17(8), 617–643. https://doi.org/10.1080/0269920031000111348
[4] Hustad, K.C., Mahr, T., Natzke, P.E.M., & Rathouz, P.J. (2020). Development of speech intelligibility between 30 and 47 months in typically developing children. Journal of Speech, Language, and Hearing Research, 63(6), 1675–1687. https://doi.org/10.1044/2020_JSLHR-20-00008
[5] Eadie, P., Morgan, A., Ukoumunne, O.C., Ttofari Eecen, K., Wake, M., & Reilly, S. (2015). Speech sound disorder at 4 years: Prevalence, comorbidities, and predictors in a community cohort of children. Developmental Medicine & Child Neurology, 57(6), 578–584. https://doi.org/10.1111/dmcn.12635
[6] Holm, A., Sanchez, K., Crosbie, S., Morgan, A., & Dodd, B. (2021). Is children’s speech development changing? Preliminary evidence from Australian English-speaking 3-year-olds. International Journal of Speech-Language Pathology, 24(4), 375–384. https://doi.org/10.1080/17549507.2021.1991474
[7] Morgan, A., Ttofari Eecen, K., Pezic, A., Brommeyer, K., Mei, C., Eadie, P., Reilly, S., & Dodd, B. (2017). Who to refer for speech therapy at 4 years of age versus who to ‘watch and wait’? The Journal of Pediatrics, 185, 200–204. https://doi.org/10.1016/j.jpeds.2017.02.059
[8] Sahih al-Bukhari 3568. Narrated Aisha (رضي الله عنها): “The Prophet ﷺ used to talk so clearly that if somebody wanted to count the number of his words, he could do so.” Graded: Sahih. https://sunnah.com/bukhari:3567
[9] Reilly, S., McKean, C., Morgan, A., & Wake, M. (2015). Identifying and managing common childhood language and speech impairments. BMJ, 350, Article h2318. https://doi.org/10.1136/bmj.h2318
[10] Law, J., Garrett, Z., & Nye, C. (2003). Speech and language therapy interventions for children with primary speech and language delay or disorder. Cochrane Database of Systematic Reviews, 3, CD004110. https://doi.org/10.1002/14651858.CD004110
[11] McLeod, S., & Baker, E. (2017). Children’s speech: An evidence-based approach to assessment and intervention. Pearson Education.
[1-Q] Qur’an 73:4. Surah Al-Muzzammil. Tafsir Ibn Kathir: tartil means giving each letter its due from its correct articulation point (makhraj) — slowly, clearly. Verified via multiple tafsir sources. https://quran.com/73/4