
Most Parents Make This Ear Infection Mistake Without Knowing It
What Every Parent Should Know About Ear Infections Before It Gets Urgent

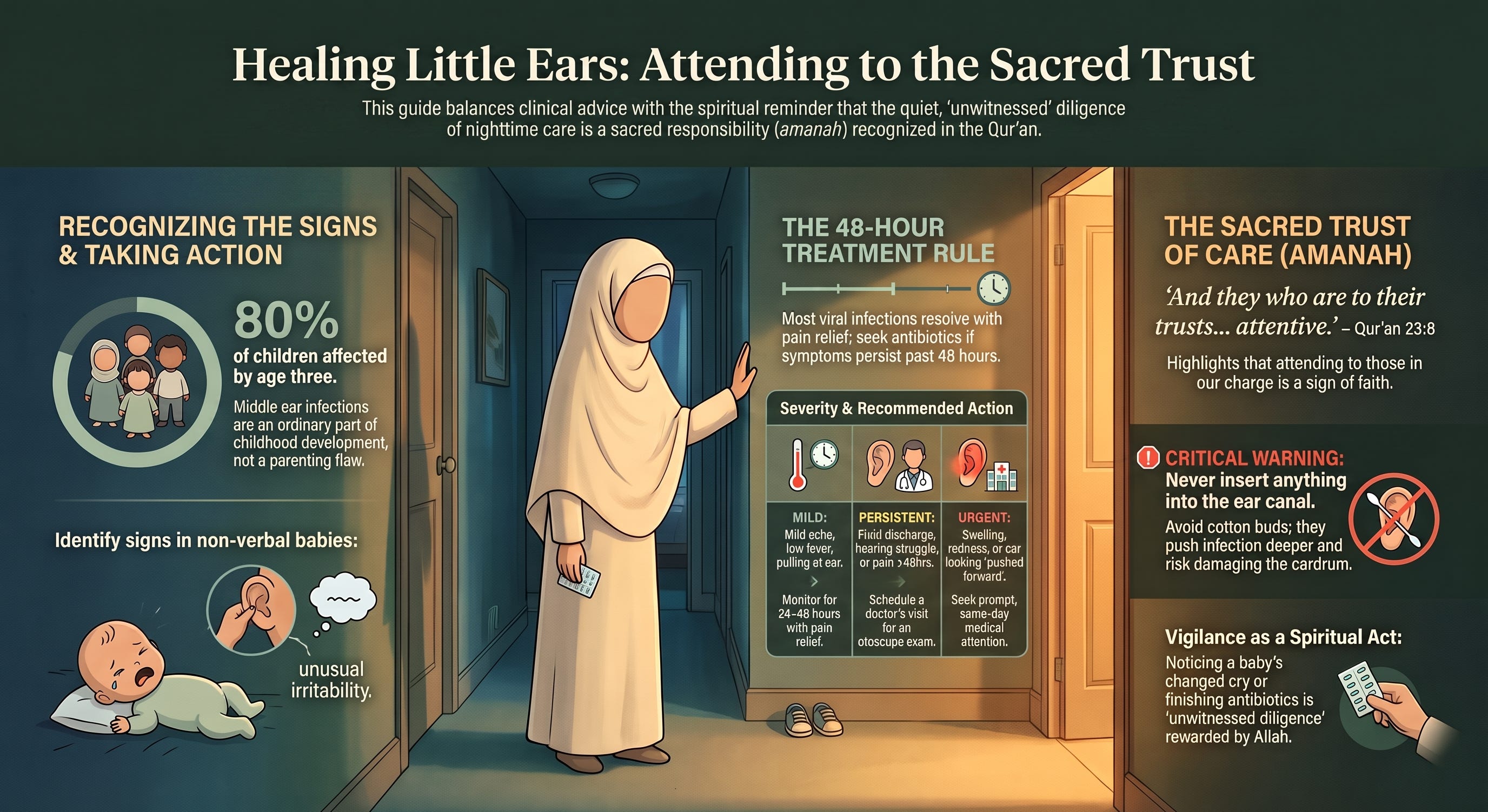
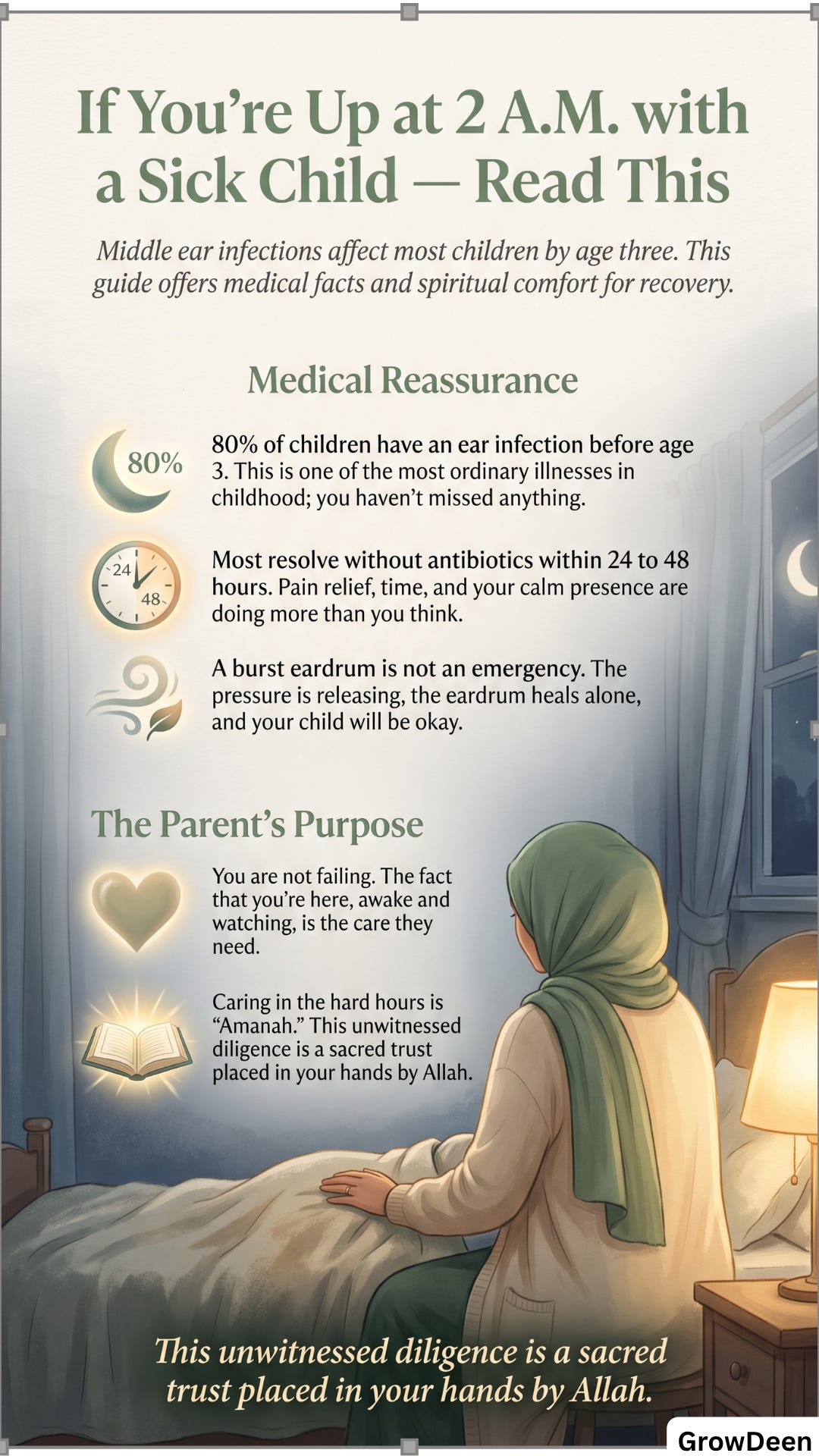
More than 80% of children have at least one middle ear infection before age three [1]. This guide shows you exactly how to recognise it, treat it, and avoid the one common habit paediatricians warn actually makes things worse.
There’s a particular kind of exhaustion that comes with a baby who won’t stop crying at 2 a.m., pulling at one ear, refusing to lie flat.
If you’ve been there, you already know how fast worry sets in. You start running through everything — is this an emergency, did I miss something, why does this keep happening.
Here’s something worth holding onto before we go any further: this is one of the most ordinary illnesses in early childhood. More than 80% of children will have had at least one middle ear infection by their third birthday [1].
You are not doing anything wrong.
I want to walk you through what’s actually happening inside your child’s ear, what to watch for, when to worry and when not to, and why a small act of ordinary parental diligence has deeper Islamic meaning than it might feel like in the moment.
Why This Guide Is Different
We go past “see a doctor.” You’ll understand exactly what’s happening behind the eardrum, why young children get this so much more than adults, and what the warning signs of something more serious actually look like.
We keep the clinical depth intact. This isn’t a stripped-down summary — you’re getting the same level of medical detail as a full clinical guide, just organised for a tired parent to actually read.
We connect the science to something Islam has always understood. A sick child’s care isn’t just a practical task. The Qur’an has a word for the quiet, unwitnessed diligence a parent shows at 2 a.m. — and it matters more than it feels like in the moment.
What’s Actually Happening in There
The medical term is otitis media — an infection in the small, air-filled space just behind the eardrum. The ear works in three connected sections: the outer ear you can see, the middle ear tucked behind the eardrum and linked by a narrow tube to the back of the throat, and the inner ear, home to the nerves that translate sound and balance. When a virus or bacteria gets into that middle section, fluid collects, pressure builds, and pain follows [2].
Young children are simply built for this to happen more easily. The tube connecting their middle ear to the throat sits shorter and flatter than an adult’s, which means fluid and germs travel there with far less resistance. That tube lengthens and angles downward as your child grows — one quiet reason ear infections become rare after the toddler years.
This is a design feature of childhood, not a flaw in your parenting.
Recognising It
Older children can usually tell you something’s wrong: an ache, a strange fullness, sounds that seem muffled. Watch too for a child who seems off balance, runs a fever, goes off their food, or turns unusually clingy and short-tempered.
Some children are in real, sharp pain. Others show almost nothing at all — which is part of why parents so often feel caught off guard.
Babies can’t report any of this. What you’ll notice instead is more crying than usual, worse when they’re lying flat — lying down changes the pressure inside the ear — and a hand that keeps finding its way to one side of the head.
Occasionally the pressure becomes too much and the eardrum ruptures. It sounds worse than it is. A small amount of thick, sometimes blood-tinged fluid appears, the pressure releases, the pain usually eases almost immediately, and the eardrum heals on its own in the vast majority of cases [3].
When Infections Keep Coming Back: Glue Ear
Repeated infections can leave behind a thick, glue-like fluid in the middle ear even after the infection itself has cleared. This is “glue ear,” and because it muffles the sound reaching the inner ear, it can cause a period of hearing loss [4].
This is the part worth taking seriously — not because any single infection is dangerous, but because hearing is how a young child absorbs language in the first place. A child straining to hear muffled sound for weeks or months at a time can fall behind in speech and understanding through no fault of their own — and can catch back up quickly once hearing is restored.
It isn’t cause for panic. It’s cause for attention.
When to See a Doctor
Take your child to a doctor if they:
Complain of earache
Have any discharge from the ear
Seem generally unwell or feverish
Appear to be struggling to hear
Keep getting infection after infection
Show swelling, redness, or an ear that looks pushed forward — this one needs prompt attention
A doctor will look inside the ear with an otoscope and may run tympanometry, a quick, painless test that measures how well the eardrum moves. If infections won’t settle or glue ear is suspected, a referral to an audiologist for a formal hearing test is common — and can be done safely at any age, including in the first year of life [5].
Treating It
Most middle ear infections are viral, and most improve on their own within 24 to 48 hours. Paracetamol or ibuprofen at the recommended dose can take the edge off pain and fever in the meantime. If pain is severe, a doctor may suggest numbing drops.
Antibiotics come into the picture when a child is still unwell and in pain after 48 hours, seems particularly unwell, or is under 12 months old — situations where a bacterial infection is more likely and less likely to resolve on its own [6].
If your child is prescribed antibiotics, finish the whole course, even once they seem better. Stopping early can let the infection creep back. Many doctors will want to see your child again once treatment is done, just to confirm things have properly cleared.
What Not to Do
Don’t put cotton wool, cotton buds, or anything else inside your child’s ear canal, including to clean discharge. It’s one of those instincts that feels helpful and does the opposite — pushing infection deeper, damaging the canal, risking the eardrum. If cleaning is needed at all, the outer ear only, with the softly twisted corner of a tissue, is enough [7].
Recurring Infections and Longer-Term Care
Some children with frequent infections or persistent glue ear need a longer course of antibiotics; others are simply monitored, since glue ear tends to clear on its own within about three months [8]. Your doctor may suggest small adjustments too — avoiding heavily chlorinated, heated pools during a run of infections is a common one.
For children whose infections won’t settle despite everything, an ear, nose and throat specialist may recommend grommets: tiny tubes placed in the eardrum that ventilate the middle ear, equalise pressure, and stop fluid building up while the child’s own tubes mature and take over [9].
What Actually Helps Prevent Them
Breastfeeding for at least the first six months is linked to fewer middle ear infections, likely a combination of the antibodies passed through milk and the different mechanics of breast versus bottle feeding [10].
As your child gets old enough, teaching them to blow their nose helps keep that ear-to-throat tube open and draining. And keeping your child away from second-hand smoke matters more than people tend to assume — smoke exposure is tied to a noticeably higher rate of ear infections, among other illnesses.
📖 Before we go further — inside the free Calm Ear Care Companion Pack, I’ve put together a red-flag quick-check card and the exact “never/always” ear care rules on one printable page. More on that in a moment.
The Trust in the Small, Unwitnessed Moments
As Muslim parents, we understand that everything involved in raising our children falls under amanah — the trusts Allah has placed in our hands. It’s easy to picture amanah as something grand: a will honoured, a promise kept, a secret guarded. Less easy to recognise it in a 2 a.m. decision about whether an earache needs a doctor visit tomorrow or tonight.
Allah says in the Qur’an: “And they who are to their trusts and their promises attentive...” [Qur’an 23:8] [11]. According to Tafsir Ibn Kathir, the word used here for trusts — amanat — is deliberately comprehensive. It covers every trust placed in a person’s charge, whether by Allah, by society, or by individuals. Ibn Kathir pairs this with the description of the hypocrite’s signs, one of which is betraying what’s been entrusted to them, to underline how seriously this attentiveness is meant to be taken.
A child’s health is exactly this kind of trust. Noticing that your baby’s crying has changed. Making the tired decision to call the doctor rather than wait and see. Finishing the full course of antibiotics even after the crying has stopped and it would be easier to let it slide.
None of this feels sacred while you’re doing it. It’s just Tuesday. But it’s precisely this kind of unwitnessed diligence — the trust nobody’s checking on but Allah — that the verse is describing.
What I find moving is how naturally this sits alongside the medical guidance already covered above. Finishing antibiotics, watching for red-flag symptoms, following up when a doctor asks you to — none of it is glamorous. All of it is attentiveness to a trust.
May Allah accept the tired, unremarkable diligence of an ordinary hard night, and make it heavier on the scale than it ever felt in the moment.
Inside the Calm Ear Care Companion Pack
If you’ve read this far, you’re the kind of parent who takes your child’s health seriously — not as anxiety, but as protective love. That tells me something beautiful about you.
Inside the Calm Ear Care Companion Pack (one comprehensive PDF, 3 pages):
Page 1: Is It Serious? A Quick-Check Card — A calm decision guide separating “mild symptoms, treat at home” from “red flags, see a doctor today,” written in plain language with no medical jargon — designed as a card you can glance at on your phone at 2 a.m. without having to think clearly.
Page 2: The Never/Always Ear Care Card — A simple two-column visual: everything to never do (cotton buds, inserting anything, ignoring discharge) beside everything to do instead (soft tissue on the outer ear only, pain relief, when to call the doctor) — so you can act confidently in under a minute, even exhausted.
Page 3: A Reminder for the Unwitnessed Nights — Featuring Qur’an 23:8 in Arabic, transliteration, and translation, paired with a short reflection on how ordinary, unglamorous diligence during a child’s illness — the phone call, the finished antibiotics, the follow-up visit — is exactly the kind of trust Allah asks believers to be attentive to. Something to read tonight, and on every ordinary hard night after this one.
This isn’t just a PDF to download and forget. It’s a tool designed to stay on your phone or your fridge — where you’ll actually use it when you need it most.
This Calm Ear Care Companion Pack is what every subscriber receives with each article. We cover the full journey of raising Muslim children, all backed by scientific research and rooted in Islamic wisdom.
If you’re a Muslim parent who wants both evidence-based guidance AND Islamic perspective, subscribe for free so future resources arrive in your inbox before you need them.
Subscribe free for parenting resources backed by both science and Sunnah — guidance so unique, you literally can’t get it anywhere else — no spam, no clutter, just resources that matter.
One Thing You Can Do Right Now
Before you close this tab: go check your bathroom cabinet. If there’s a box of cotton buds sitting near the baby wipes or bath supplies, move it somewhere it’s clearly not “for ears.” That’s it. That’s the whole action. Small, but it’s exactly the habit this article is asking you to break.
Share This With Someone Who Needs It
Think of one person right now: the friend whose toddler just had their third ear infection this year, the sister who texted you at midnight asking if she should be worried, the new mother in your family who’s about to hit the age where this becomes common.
This article could save them a frightening, uncertain night. Share it with them today — not because you’re being preachy, but because you care. Sometimes the most loving thing we can do is pass along knowledge before it’s needed.
Frequently Asked Questions
Q: How can I tell if my baby has an ear infection if they can’t talk yet?
A: Watch for more crying than usual — especially when lying flat, since that changes ear pressure — along with a hand or fist that keeps returning to one ear, fever, and going off feeds. See “Recognising It” above for the complete picture.
Q: Can a middle ear infection go away without antibiotics?
A: Yes — most are viral, and most clear on their own within 24–48 hours with pain relief alone [6]. Antibiotics become relevant if pain persists past 48 hours, your child is under 12 months, or they seem particularly unwell.
Q: Is it ever okay to clean inside my child’s ear with a cotton bud?
A: No — never insert anything into the ear canal, even to clean discharge [7]. Gently wipe the outer ear only with a soft tissue.
Q: What’s the difference between a regular ear infection and glue ear?
A: A regular infection is an active infection that typically resolves within days. Glue ear is thick fluid that lingers in the middle ear after repeated infections and can cause temporary hearing loss even once the infection itself is gone [4]. It usually clears within about three months.
Q: Will my child need grommets?
A: Only a small proportion of children with frequent, unresolving infections or persistent glue ear are referred for grommets — tiny tubes an ENT specialist places to ventilate the middle ear while your child’s own tubes mature [9]. Most children never need this.
Q: Does breastfeeding actually reduce ear infections?
A: Yes — breastfeeding for at least six months is associated with fewer middle ear infections, likely through both antibody transfer and feeding mechanics [10]. It’s one of several practical prevention steps covered above.
Q: When is an ear infection a real emergency?
A: Seek prompt care for swelling, redness, or an ear that looks pushed forward — these can signal a spreading infection and need same-day attention, unlike the far more common mild earache that improves within 48 hours.
References
[1] Danishyar, A., & Ashurst, J.V. (2022). Acute otitis media. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK470332
[2] Kerschner, J.E., & Preciado, D. (2024). Otitis media. In Nelson Textbook of Paediatrics (22nd edn, Chapter 680). Elsevier.
[3] Casselbrant, M.L., & Mandel, E.M. (2015). Acute otitis media and otitis media with effusion. In Cummings Pediatric Otolaryngology (pp. 209–227). Saunders Elsevier.
[4] Schilder, A.G.M., Rosenfeld, R.M., & Venekamp, R.P. (2021). Acute otitis media and otitis media with effusion. In Cummings Pediatric Otolaryngology (2nd edn, pp. 210–227). Saunders Elsevier.
[5] Steele, D.W., Adam, G.P., Di, M., Halladay, C.H., Balk, E.M., & Trikalinos, T.A. (2017). Effectiveness of tympanostomy tubes for otitis media: A meta-analysis. Pediatrics, 139(6). https://doi.org/10.1542/peds.2017-0125
[6] Coker, T., Chan, L., Newberry, S., Limbos, M., Suttorp, M., Shekelle, P., & Takata, G. (2010). Diagnosis, microbial epidemiology, and antibiotic treatment of acute otitis media in children: A systematic review. JAMA, 304(19), 2161–2169. https://doi.org/10.1001/jama.2010.1651
[7] The Royal Children’s Hospital (RCH). (2021). Clinical practice guidelines: Acute otitis media. https://www.rch.org.au/clinicalguide/guideline_index/Acute_Otitis_Media/
[8] Leach, A.J., & Morris, P.S. (2006). Antibiotics for the prevention of acute and chronic suppurative otitis media in children. Cochrane Database of Systematic Reviews, 4, CD004401. https://doi.org/10.1002/14651858.CD004401.pub2
[9] van den Aardweg, M.T.A., Schilder, A.G.M., Herkert, E., Boonacker, C.W.B., & Rovers, M.M. (2010). Adenoidectomy for otitis media in children. Cochrane Database of Systematic Reviews, 1, CD007810. https://doi.org/10.1002/14651858.CD007810.pub2
[10] Coleman, C., & Moore, M. (2008). Decongestants and antihistamines for acute otitis media in children. Cochrane Database of Systematic Reviews, 3, CD001727. https://doi.org/10.1002/14651858.CD001727.pub4
[11] Qur’an 23:8. Tafsir Ibn Kathir, Surah Al-Mu’minun, verse 8. Available via alim.org and quran.com.